Blakemore Tube Placement for Massive Upper GI Hemorrhage - a podcast by Scott D. Weingart, MD FCCM
from 2013-10-13T19:31:45
In recent lectures, I talk about a life-saving Blakemore Tube placement. I suspect some of you may need a reminder of the intricacies of this device, so I made a video and cheat-sheet.
Improved HD Video
Jess Mason took the moves in my original video and had it recorded professionally
Securement using ETAD Device
Jess Mason made this nice video on how to secure the Blakemore
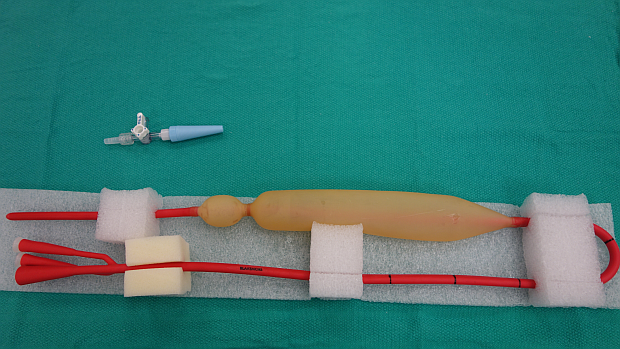
What you need:
* Blakemore
* Salem Sump
* 60 ml Luer-lock Syringe
* 60 ml Slip-tip Syringe
* 2 x-mas tree to male luer lock converters
* 3 three-way stopcocks
* 3 medlock caps
* Surgilube
* Roller-bandage
* 1 1-liter bag of crystalloid
* Optional: 2 Hollister ETAD ET tube securing devices
* Possibly: Laryngoscope, Magill Forceps
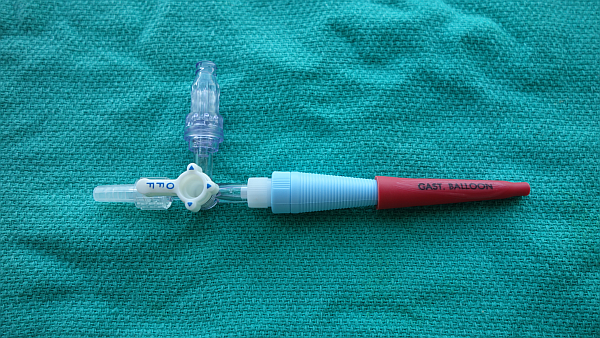
Gastric Port
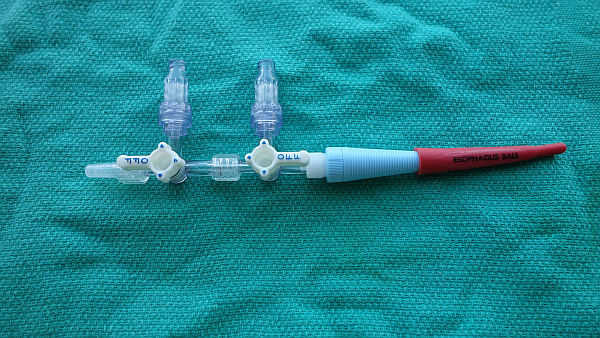
Esophageal Port
How to Do it:
* Patient should be intubated and the head of the bed up at 45 degrees.
* Test balloons on Blakemore and fully deflate. Mark salem sump at the 50 cm mark of the Blakemore with the tip 2 cm above gastric balloon and then 2 cm above esophageal balloon.
* Insert the Blakemore tube through the mouth just like an NGT. You may need the aid of the laryngoscope and sometimes McGill forceps. Make sure the depth-marker numbers face the patient’s right-side.
* Stop at 50 cm. Test with slip syringe while auscaltating over stomach and lungs. Inflate gastric port with 50 ml of air or saline.
* Get a chest x-ray to confirm placement of gastric balloon in stomach.
* Inflate with additional 200 ml of air (250 ml total)
* Apply 1 kg of traction using roller bandage and 1 liter IV fluid bag hung over IV pole. Mark the depth at the mouth. The tube will stretch slightly over the next 10 minutes as it warms to body temperature.
* After stretching, the tube may be secured to the ETAD tube holder.
* Insert the salem-sump until the depth marked gastric is at 50 cm on the Blakemore. Suction both Blakemore lavage port and salem sump. You may need to wash blood clots out of the stomach with sterile water or saline.
* If bleeding continues, you will need to inflate esophageal balloon.
* Pull salem sump back until the esoph. mark is at the 50 cm point of the Blakemore. Attach a manometer to the second 3-way stopcock on the esophageal port of the Blakemore. Inflate to 30 mm Hg. If bleeding continues, inflate to 45 mm Hg.
* Consider switching traction to Hollister ETAD Device.
Here is a cheat sheet for Blakemore Placement in PDF Form
How to Build a Simulator
Paper from JEM
Bougie Aided Placement Technique by Whitford
Questions to be answered?
* Can ultrasound obviate the need for radiographic confirmation prior to inflation? One letter to the editor says yes, but the image doesn't seem to confirm anything. (Emerg Med J 2006;23:487)
{kind=link}
{kind=link}
{kind=link}
Further episodes of EMCrit Podcast
Further podcasts by Scott D. Weingart, MD FCCM
Website of Scott D. Weingart, MD FCCM