EMCrit Podcast 12 – Trauma Resus: Part I - a podcast by Scott D. Weingart, MD FCCM
from 2009-10-14T04:10:05
Thought we'd talk about some trauma stuff, specifically the resuscitation of the critically ill hemorrhagic shock patient.
There is much to discuss, so this will be a multi-episode affair.
Today, we'll concentrate on the Lethal Triad and BP Goals.
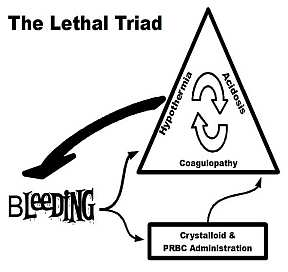
Lethal Triad
The picture says it all.
Bleeding causes acidosis, hypothermia, and coagulopathy. Then the cycle begins as they all beget each other. If this continues for too long, it is irreversible.
We can iatrogenically make things worse by keeping our patients exposed and infusing ice cold fluids and products. By diluting their existing clotting factors and platelets with too much fluid and red cells. And by not ensuring adeqaute perfusion to counter acidosis.
BP Goals
Your goal is a MAP of 65. This is not hypotensive resus, which is still not proven. It is normotensive resuscitation; beyond 65, no additional benefts will be seen, but you do risk increased bleeding and dilutional coagulopathy.
If MAP < 65 - give fluids/products
If MAP > 65 - check perfusion
there are monitors for this such as NIRS measurement of thenar eminence, but at this stage, I recommend using the presence of a nice strong pulse and warm hands.
MAP > 65 & Good Perfusion-stand tight
MAP > 65 & Bad Perfusion-give fentanyl 20-25 mcg
why fentanyl? b/c taking away pain and fear will limit endogenous catecholamines and the pt's bp will drop slightly from vasodilation. Now give fluids/products to take the MAP to > 65.
Here are the articles
resus of crit ill trauma patients
damage_control_anesthesia
Next Time: Massive Transfusion Protocols
{kind=link}
Further episodes of EMCrit Podcast
Further podcasts by Scott D. Weingart, MD FCCM
Website of Scott D. Weingart, MD FCCM