EMCrit Podcast 17 – Reversal of Anti-coagulant and Anti-platelet Drugs in Head Bleeds - a podcast by Scott D. Weingart, MD FCCM
from 2010-01-12T21:53:51
So you have a patient with intracranial bleeding or you have a high pre-ct suspicion of intracranial bleeding and they are taking coumadin, aspirin, or clopidogrel. Should you reverse them? If so, how?
What if the CT is negative? Can you just discharge these patients as soon as they have a negative CT?
In this episode of the EMCrit Podcast, I discuss reversal of anti-coagulant drugs & anti-platelet medications, with particular emphasis on the prothrombin complex concentrates (PCC). I also touch on how to disposition these patients if their initial CT scan is negative.
Reversal Meds
Here are sample guidelines for drug reversal:
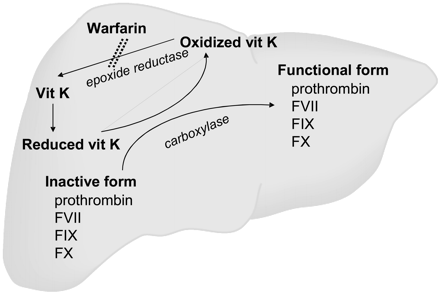
Warfarin
Any patient with a history of recent warfarin use, with an INR > 1.5 should immediately receive:
1. Vitamin K 10 mg IVPB over 10 minutes (monitor for hypotension / anaphylaxis) &
2. 50 units/kg of Prothrombin Complex Concentrate (Bebulin or Profilnine) Administer over 20 minutes.
• If PCC unavailable, give 15 cc/kg of FFP
Repeat INR 10 minutes after completion of infusion
Liver failure with known coagulopathy or elevated PT or INR •1.5
1. Vitamin K 10 mg IV over 10 minutes (monitor for hypotension / anaphylaxis) &
2. 50 units/kg of Prothrombin Complex Concentrate (Bebulin or Profilnine) &
3. 2 units of FFP
• If PCC unavailable, give 15 cc/kg of FFP total
Reversal of Platelet Dysfunction: For any patient with antiplatelet (Aspirin, Aggrenox or Clopidogrel) used in last 24 hours administer:
1. dDAVP 0.3 mcg/kg x 1 (20 mcg in 50 cc NS over 15-30 minutes) &
2. 1 donor pack platelets (~6 units)
Review Article of Vitamin K antagonist reversal (Critical Care 2009, 13:209)
Review Article on PCCs (European Journal of Anaesthesiology 2008; 25: 784–789)
Recent Study on DDAVP for Aspirin (Journal of Trauma 2020;88(1);80-86
CT Negative after Head Trauma while on Anti-coagulants or Anti-plt Meds
One man's jury-rigged approach:
Minor head trauma (the definition of this in the anticoagulant literature seems to be different than most other head trauma lit, they actually define minor as NO LOC and NO AMNESIA, just a bop to the head)
* Most folks would still say scan these patients once and then observe for 6 hours. A few would say just observe, a very few would say admit for 24 hours. I watch them for 6 hours and then get the CT scan.
Head trauma with LOC, but GCS 15
* definitely scan, definitely observe at least 6 hours, most would say either rescan or admit for 24 hours
Head trauma with LOC, but GCS < 15
* scan, almost certainly admit for 24 hours, probably rescan prior to d/c
Not great literature support for any of this, here are some studies to get you started:
Delayed Posttraumatic Acute Subdural Hematoma in Elderly Patients on Anticoagulation (Neurosurgery 58:851-856, 2006)
Low Dose ASA led to secondary bleeding not seen on initial CT in patients with normal neuro exams (J Trauma 2009 67(3):521)
Update:
From EM:RAP Aug 2013
Nishijima DK et al. Immediate and delayed traumatic intracranial hemorrhage in patients with head trauma and preinjury
warfarin or clopidogrel use. Ann Emerg Med. 2012 Jun;59(6):460-8.
o A prospective, observational study at 2 trauma centers and 4 community hospitals. Most of these patients were community
{kind=link}
Further episodes of EMCrit Podcast
Further podcasts by Scott D. Weingart, MD FCCM
Website of Scott D. Weingart, MD FCCM