EMCrit Podcast 226 – Airway Update – Bougie and Positioning - a podcast by Scott D. Weingart, MD FCCM
from 2018-06-13T14:26:54
Bougie First?
A recent RCT from Hennepin1 by Driver et al. evaluated the effect of bougie use on first pass success. This adds to a prior retrospective study by the same group.2 These studies lend support to a practice that many of us have already adapted--bougie first intubation.
Few things on the bougie stuff
Some bougies are too short & this leads to A LOT of their downsides (RCT used a 70 cm bougie, as opposed to the 60cm bougie that I have)
Most bougies don't retain their shape, which is a shame b/c the airways where you most need the bend to stay are the ones that are least likely to tolerate multiple removals to reshape. Levitan bougie should solve this
We cannot conflate the Hennepin article with preloading the bougie
Technique
* A discussion is in the episode and 2-person vs. 1 person
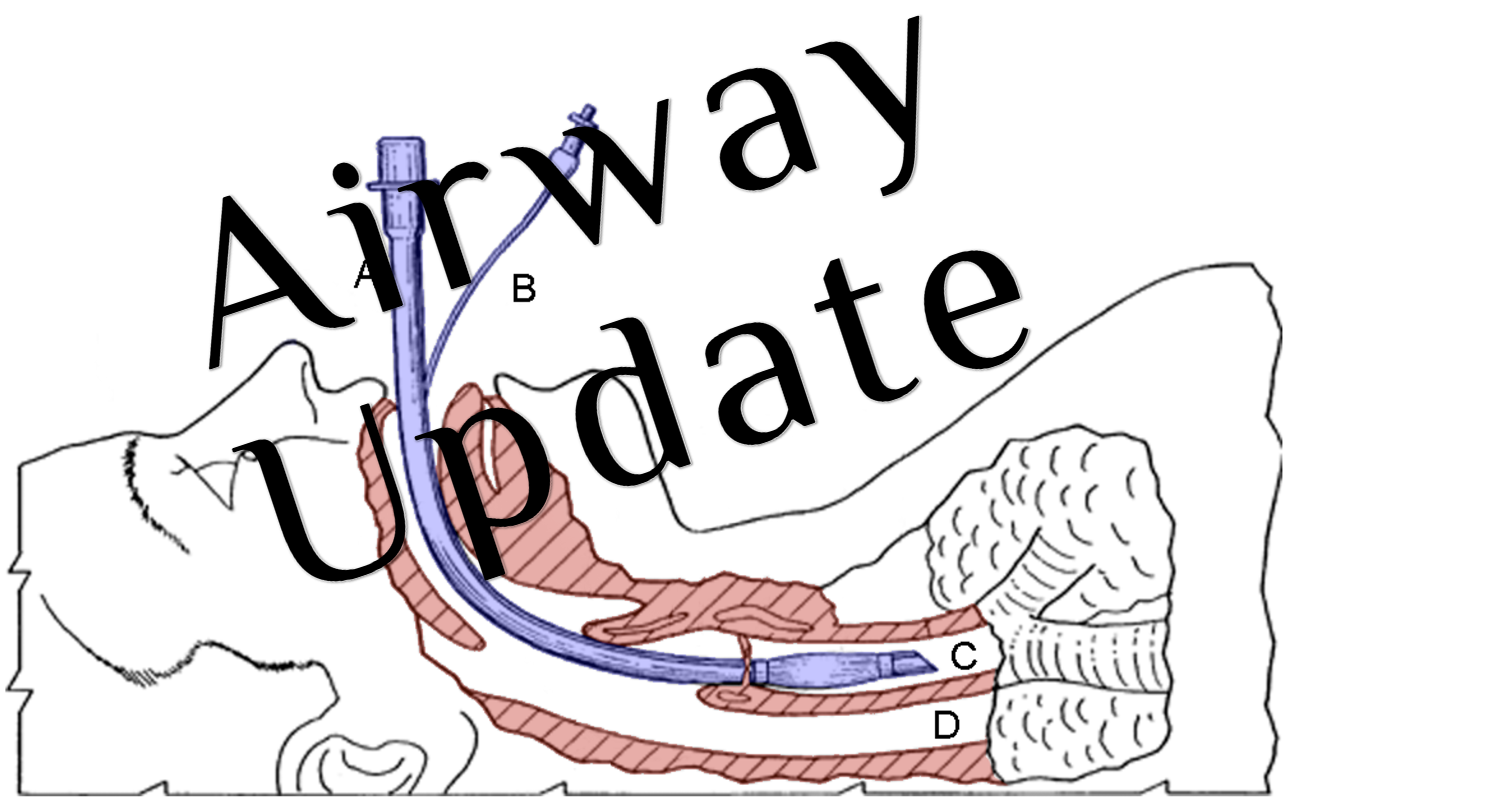
Can You Advance an ETT over a bougie without having someone grab the proximal end first??
* Listen to the episode and let me know what you think
How to know the bougie is in when used in a C/L 3 view
* Clicks - I find this unreliable
* Hold-Up - as long as this is done gently, it is fantastic
* Laura Duggan recommends: A trained assistant with gentle thumb on one side, two fingers on the other of trachea at the sternal notch is priceless to confirm placement without the need for the 'hang up test'
What about the Pre-Load Techniques?
See this poster for one bench eval
VBM S-Guide
* Video for S-Guide
I'd also like to see their METTS stylet. Go to VBM Medical to see these.
Snail Trail for Bougie Bending
from3 though I actually put the circle closer to the tip
Also See
* Bougie Vids
* EMNerd on the Bougie RCT
* Kovacs on why he doesn't like the D-Grip
* ETT vs. Railroad Bougie vs. Preload Bougie
* Sal on Driver's first study
Update
* This is the highest FPS I have seen using CMAC and Frova on all intubations4
Positioning
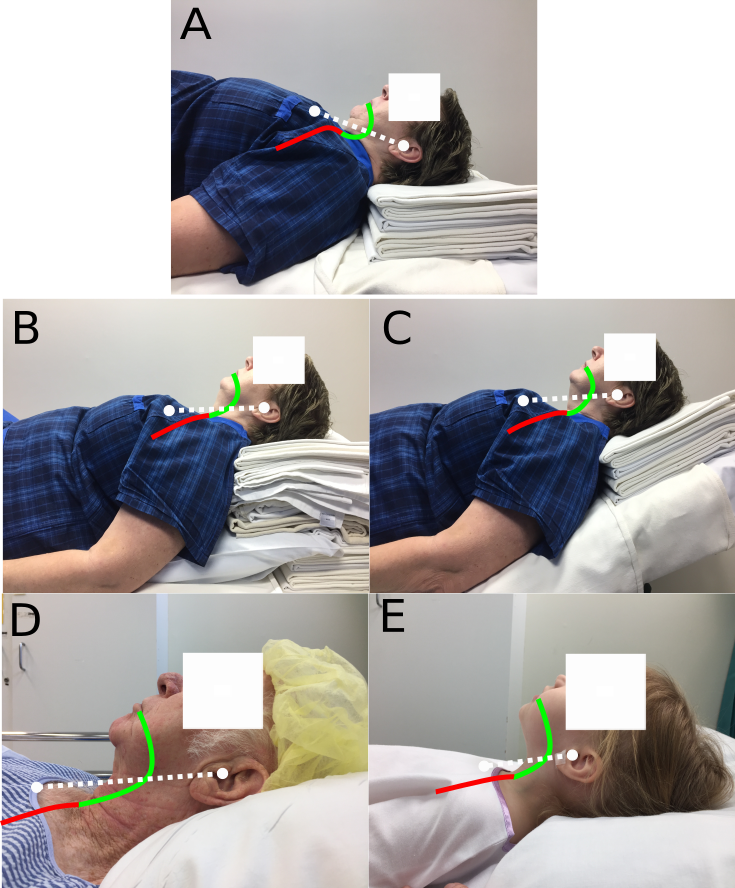
stand behind the patient
lift their head
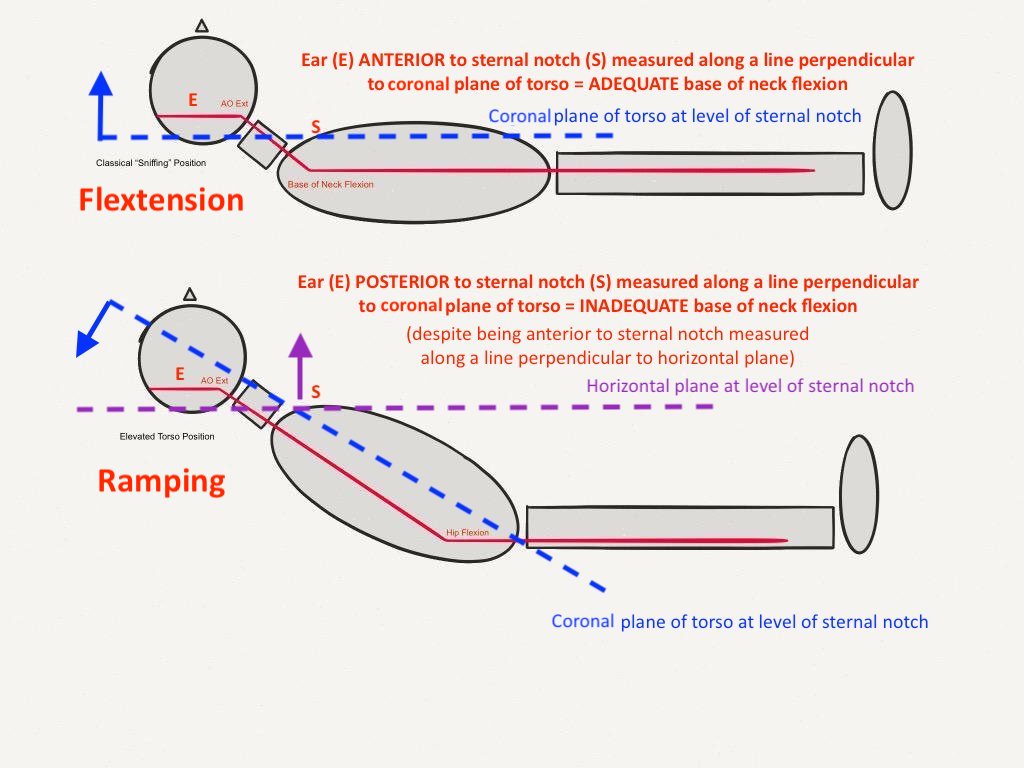
and push their head towards their feet (causing base of neck flexion)
until their ear holes (ext auditory meatus) are at or higher than the level of their sternal line (sternal notch to xiphoid process)
while constraining the face plane to stay parallel to the ceiling
then padding under head & shoulders until this position is maintained
Semler et al.5 showed Ramping is worse, however you'll need to listen to the podcast to understand what that means.
Flextension by Chrimes
Chrimes on Positioning
Greenland on Positioning
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Further episodes of EMCrit Podcast
Further podcasts by Scott D. Weingart, MD FCCM
Website of Scott D. Weingart, MD FCCM