EMCrit Podcast 244 – Incredibly Important Wrinkles to Titrated Vasopressors during CPR in Cardiac Arrest - a podcast by Scott D. Weingart, MD FCCM
from 2019-04-15T14:10:01
In episode 130 of the podcast and in many subsequent discussions, I have advocated for femoral-artery-monitoring during cardiac arrest to allow titrated use of vasopressors. Many of my colleagues in the advanced resuscitation community have a similar practice. In 2013, the AHA has released an advanced practice guideline recommending the same practice.1
But...
What if the diastolic blood pressure number shown on the monitor is the WRONG PRESSURE. That is the contention of our guest today:
[su_box title="Today's Guest"]Per-Olav Berve is a Norwegian anaesthesiologist who works for the Oslo air ambulance and in-hospital at the Oslo University Hospital. He is currently wrapping up a PhD on CPR physiology, focusing on multimodal monitoring. His main project is a OHCA study on mechanical active compression-decompression CPR. (Bio from scanFOAM).[/su_box]
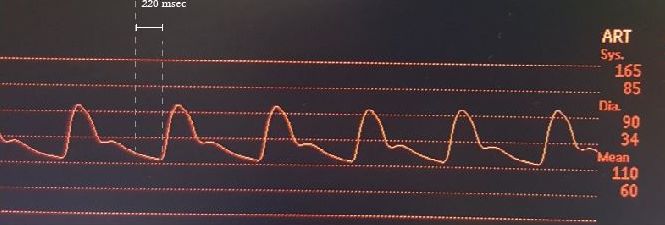
It seems the machine picks the DBP that is the lowest point between systoles. This works well with waveforms generated by the normal cardiac compression. During CPR, however the lowest point (decompression phase nadir) actually represents the reformation of the aortic outflow tract after it has been compressed. This generates a brief negative pressure which can give extremely low pressures. If you use this as your DBP you will be steered in exactly the wrong direction--the better the cpr and the more pronounced the vascular tone, the lower this number will be.
Image from PO Berve
In the arterial wave form image above, Point A is a DBP of zero. This is the number that will appear on the monitor; this number can actually be negative. In the past, I would be rezeroing the transducer thinking it must be in error. And when I spoke about refractory vasoplegia, it was because of this number. What we need to be looking at is Point B, the point just before the systolic upstroke--this is the true DBP to titrate your vasopressors according to PO. The better the CPR and the higher the vasomotor tone, the lower Point A and the higher Point B will be. So as we are doing better, we will see lower and lower DBPs if we go by the displayed numbers.
Here is a normal waveform from an actual beating heart as contrast:
Solutions
You must visualize the waveform rather than looking at the computer-generated DBP
* Change displayed waveforms to 10 sec. if possible
* Auto-Wave (match the top and bottom of the scale to the actual waveform parameters) to make the waveforms as big as possible
* If your machine has a line that can be set to a pressure, put it at 40 mm Hg and then just look to see if the beginning of the systolic upstroke is above this line
The Full Lecture from the Big Sick
ScanFOAM has an amazing post with PO's full lecture, slides, and all the references from the lecture.
* PO Berve on Waveforms during Cardiac Arrest from scanFOAM
The Paradis et al. Papers
* 1989 Paper2
* 1990 Paper3
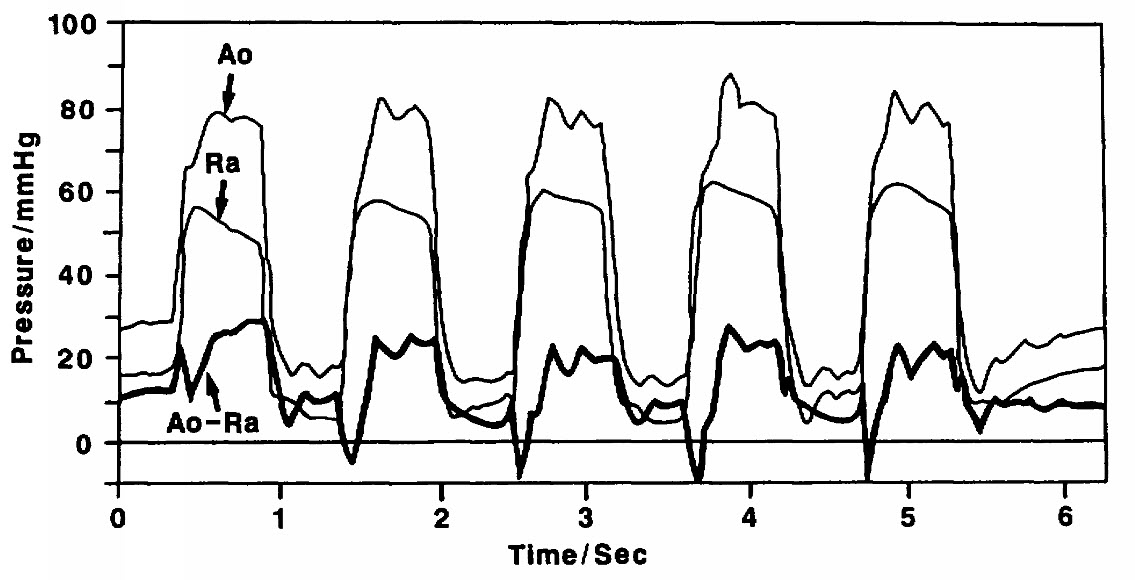
Superimposed Aortic and Right Atrial Waveforms
from Paradis et al. 1989
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Further episodes of EMCrit Podcast
Further podcasts by Scott D. Weingart, MD FCCM
Website of Scott D. Weingart, MD FCCM