EMCrit Podcast 247 – The Dissociated Awake Intubation with my buddy, Ketamine - a podcast by Scott D. Weingart, MD FCCM
from 2019-05-16T17:09:12
Today, we talk about the theory and practice of the Dissociated Awake Intubation. This technique allows the rapid provision of an intubatable patient while preserving spontaneous respirations.
A few days ago I posted George Kovacs' thoughts on the matter.
* George Kovacs on KFI
This was in response to a blog post by frenemy of the show and brilliant airway tactician, Reub Strayer.
* Ketamine-Only Breathing Intubation (KOBI)
What is Dissociated Awake Intubation?
I coined this term to describe the administration of a dissociating dose of ketamine to allow a patient to be intubated for many of the same circumstances as the traditional topical awake approach.
This is theoretically distinct from the idea of using ketamine in a sedative-only intubation. The two ideas are separated by the intent, with the former subbing for a topical awake and the latter for a RSI, in systems where for whatever reason, paralytic can be used. In practice, they look the same--it is often the users that look different.
Kovacs has used the term ketamine facilitated intubation to encompass both uses. This post and podcast only deal with dissociated awake.
Awake Intubation Posts
* Emergency Awake Topicalized (EAT) Intubation – An Awake Intubation Update
* Podcast 194 – Definitive Emergent Awake Intubation with George Kovacs
Why Awake Intubation?
If an airway is predicted to be difficult, consider an awake approach. This predicted difficulty could be an anatomic. It could also be physiological: namely Hemodynamics Kills, Oxygenation Kills, or pH Kills. When there is a combination of two or three of these elements, awake becomes almost a must.
Awake vs. RSI
RSI and awake are tradeoffs
* RSI gives you the easiest laryngoscopy/tube delivery at the expense of safe time for intubation
* Awake gives you a markedly harder laryngoscopy/tube delivery rewarded by a markedly extended safe intubation time
You must be a much better intubator to perform an awake laryngoscopy and tube delivery.
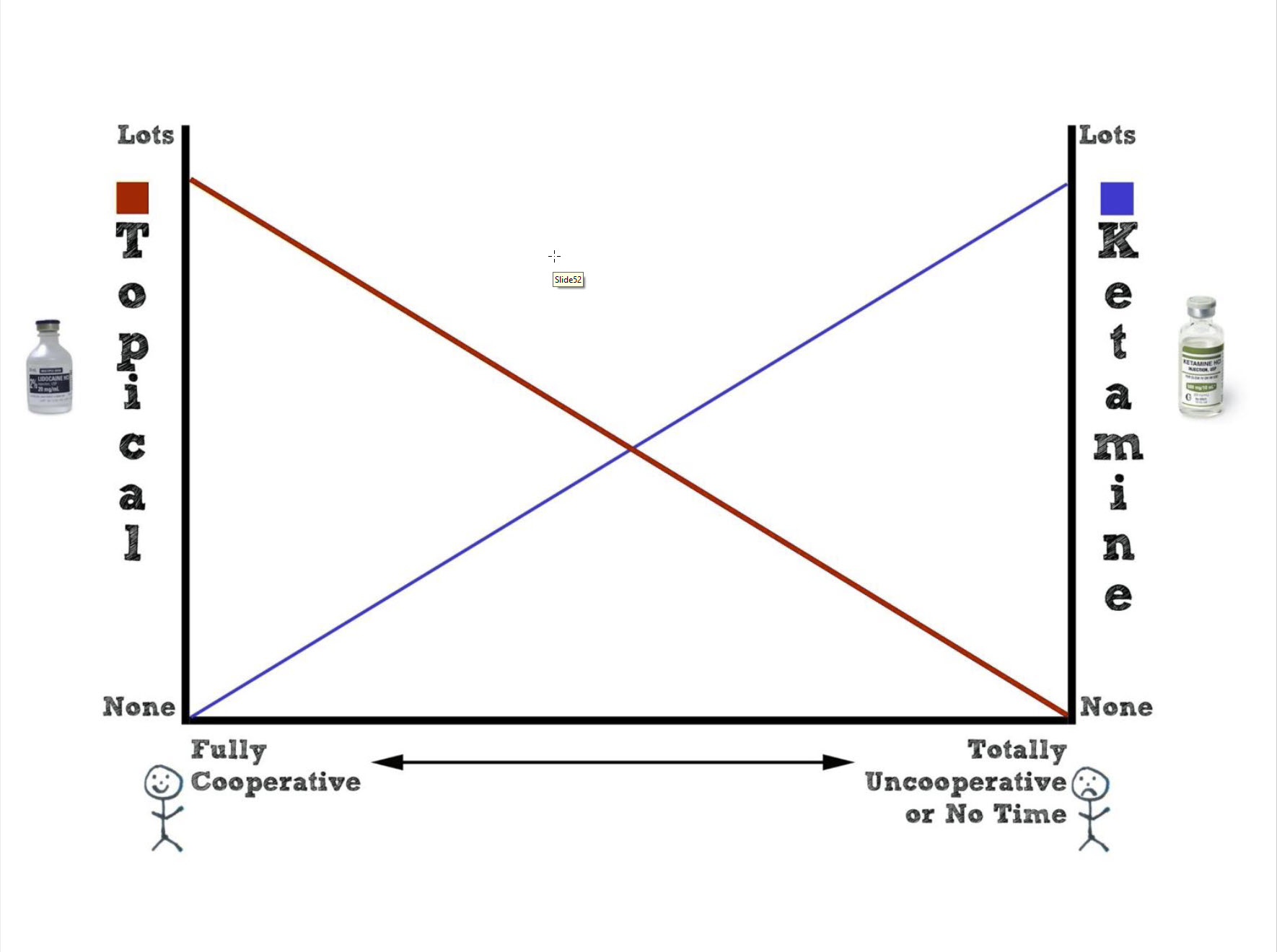
Topicalized vs. Dissociated Awake
In some cases you will try topical first, and then when the pt won't cooperate or you can't adequately topicalize, that will push you to dissociation. However, there are definitely a group of patients who I will choose primary dissociated awake. It comes down to cognitive bandwidth.
Nuts and Bolts of the Technique
* Give small aliquots of ketamine every 15 sec. or so until dissociation (25 mg at a time
* Have everything ready for RSI and failed airway, including paralytics prepared and ready before first dose of ketamine
* I still topicalize
Awake Intubation from George's Online Textbook
Kovacs AIME Airway Textbook (Infinity Edition) - Awake Intubation Chapter)
Now on to the Podcast...
{kind=link}
Further episodes of EMCrit Podcast
Further podcasts by Scott D. Weingart, MD FCCM
Website of Scott D. Weingart, MD FCCM