EMCrit Wee – A Theoretical Model of the Pathophysiology of COVID-19 with Farid Jalali (Not a Single Thing Verified–Pure Musings) - a podcast by Scott D. Weingart, MD FCCM
from 2020-05-18T13:23:43
Today on the podcast, my guest lays out a theoretical framework for the pathophysiology of the lung effects of COVID-19.
Farid Jalali
Dr. Farid Jalali received his Medical Degree from West Virginia University School of Medicine in 2012. He completed his postgraduate training in Gastroenterology at the University of California, Irvine Medical Center in 2018. Dr. Jalali has had extensive training and experience in diagnosing and treating a broad spectrum of GI and Liver disorders. He has a special focus on cancer prevention and spends a great deal of time educating and helping patients on how to prevent cancers in the GI tract and Liver. [@farid__jalali]
Pathophysiology
Potential Treatments
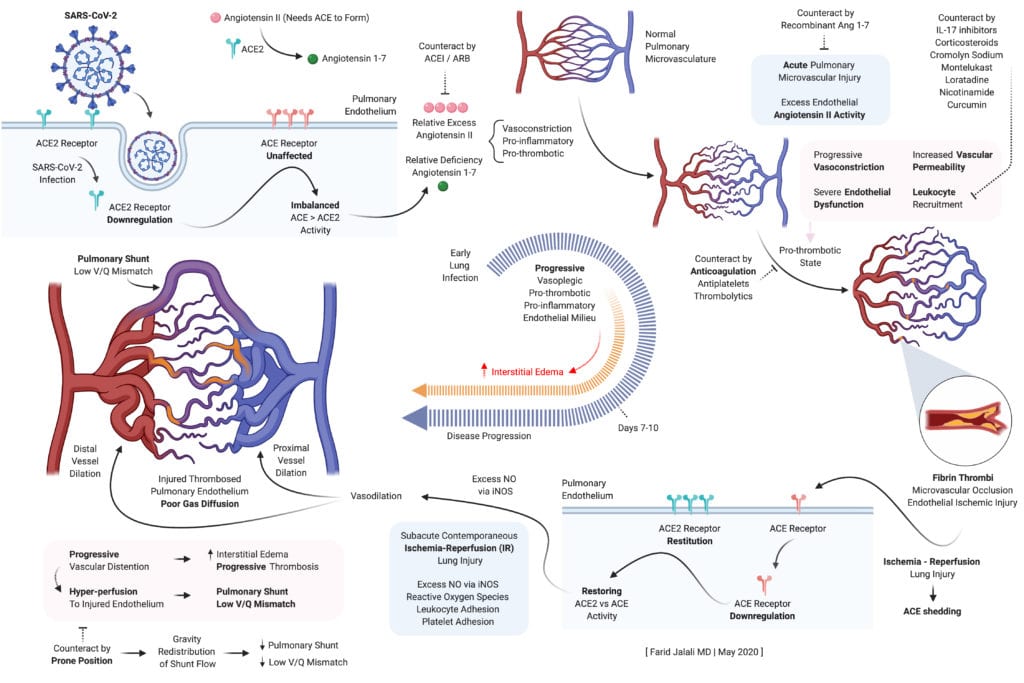
Slides from the Presentation
* Farid Jalali COVID-19 Pathophys
Take Home Points from the Talk
* Early endothelial stabilization, before hypoxia sets in, is key to prevent SARS-CoV-2 induced, excess Angiotensin II mediated, intense alveolar capillary vasoconstriction as well as the concomitant pro-inflammatory, pro-thrombotic endothelial milieu, all of which form the basis of lung
injury in COVID19.
* Once hypoxia sets in, supportive care should include early and aggressive endothelial stabilization interventions, properly dosed anticoagulation to prevent lung microvascular thrombi, HFNC, and awake prone position to redistribute flow away from the forming dorsal-predominant intrapulmonary shunts.
* Alveolar capillary microvascular thrombi are not a pre-requisite for the severe lung injury in COVID19, but are a clear step in the wrong direction if allowed to be formed.
* Lung's natural and physiologic protective response to SARS-CoV-2 induced alveolar capillary vasoconstriction and dead-space ventilation is characterized by alveolar hypocapnic bronchoconstriction at the level of the alveolar ducts to reduce a harmful alveolar expansion in these affected capillaries.
* Naturally, unaffected capillaries and corresponding alveoli will have a higher redistribution of ventilation, will exchange more CO2 into alveolar space, and will therefore have hypercapnic bronchodilation.
* This redistribution keeps the lung compliance preserved in the initial lung injury characterized mainly by dead-space ventilation, forming intrapulmonary shunts, without significant interstitial or alveolar edema.
* Compensatory lower inspiratory volumes characterize the patient's response, associated with higher respiratory rate, and "shallow rapid breaths" without distress. [this has not been my experience--EMCrit]
* This lower inspiratory volume is needed to prevent expansion of alveoli in the affected vasculopathic areas, as inappropriate expansion compounds the vasoconstriction in these affected alveolar capillaries.
* This will result in a compensatory tendency to develop hypocapnea on blood gas analysis, often concomitant with hypoxia as intrapulmonary shunts also begin to form as lung injury progress.
* Higher lung volumes, and positive pressure ventilation, disturb the fine balance maintained physiologically in the ventilatory redistribution pattern of the COVID1 9 lung, between high V/Q mismatch areas (poor perfusion, compensatory reduced ventilation to protect against the vasculopathy) and the compensating lower V /Q areas that safely receive higher ventilation in return.
* Therefore, mechanical ventilation may result in worsening of dead-space ventilation by constricting alveolar cap...
{kind=link}
{kind=link}
{kind=link}
Further episodes of EMCrit Podcast
Further podcasts by Scott D. Weingart, MD FCCM
Website of Scott D. Weingart, MD FCCM