EMCrit Wee – The Targeted Temperature Trial Changes Everything - a podcast by Scott D. Weingart, MD FCCM
from 2013-11-18T20:28:29
The TTM Trial was just published today in the NEJM (Nielsen et al. Targeted Temperature Management at 33°C versus 36°C after Cardiac Arrest NEJM 2013;epub Nov 17, 2013)
For my take and the take of Jon Rittenberger, come to the 2nd TTM Post
but even more important is to hear from the primary author himself: Niklas Nielsen on the TTM Trial
Study Design
International multicenter RCT
Inclusion criteria: Age >= 18 years, out-of-hospital cardiac arrest of presumed cardiac cause, unconsciousness (Glasgow Coma Score <8) after sustained return of spontaneous circulation (ROSC) (20 minutes of circulation).
Exclusion criteria: Conscious patients, pregnancy , out-of-hospital cardiac arrest of presumed non-cardiac cause, cardiac arrest after arrival in hospital, known bleeding diathesis, suspected or confirmed acute intracranial bleeding, suspected or confirmed acute stroke, temperature on admission <30°C, unwitnessed asystole, persistent cardiogenic shock, known limitations in therapy, known disease making 180 day survival unlikely, known pre-arrest cerebral performance category 3 or 4, >240 minutes from ROSC to randomisation.
Primary outcome: Survival to end of trial (at least 180 days).
Secondary outcomes: Composite outcomes of all-cause mortality and poor neurological function (Cerebral Performance Category (CPC) 3 and 4 and modified Rankin Scale (mRS) 4 and 5) at 180 days. All - cause mortality and CPC and mR S at 180 - days. Adverse events: Bleeding, pneumonia, sepsis, electrolyte disorders, hyperglycaemia, hypoglycaemia, cardiac arrhythmia, renal replacement therapy.
Tertiary outcomes: Complete neurological recovery. Best neurological outcome during trial perio d. Quality of life according to SF - 36. Biomarkers at 24, 48 and 72 hours
Intervention: The core body temperature will be set as quickly as possible at the predefined target temperature, according to intervention allocation, with 4°C intravenous solutions, 43 ice - packs 8, 44 and commercially available cooling devices 45 at the discretion of the treating physician . The target core temperature is then maintained for 24 h. After the maintenance period core temperature is gradually raised to normothermia of 37°C during 8 hours with a rewarming rate of 0.5°C/hour in both groups. Body temperature is then maintained at normothermia 37 ±0.5°C until 72 hours from sustained ROSC in both treatment groups, as long as the patient is in the ICU, using pharmacological treatment and temperature management systems when applicable
See all of the nitty-gritty in the appendix
rewarmed at 0.5 C/hr and then induced normothermia (37.5 C) for 36 hrs post arrest
Nonblinded to temp allocation, but neuro assessment was blinded
fluids icepacks surface and intravasc cooling-- 1/4 intravasc and rest surface
900 pts give 90% power to detect 20% difference
80% shockable, 12% asystole
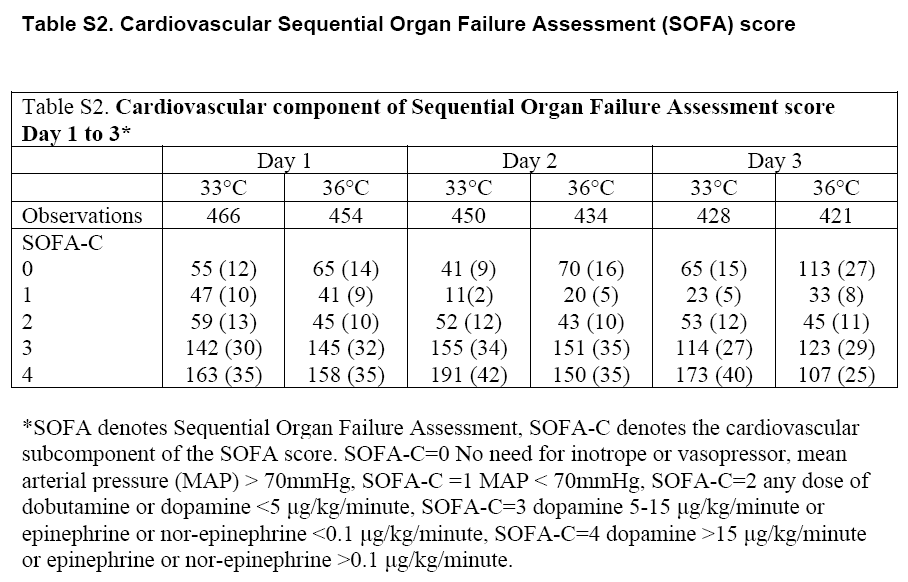
Table S2 - SOFA-C Scores in the first 72 hours
*SOFA denotes Sequential Organ Failure Assessment, SOFA-C denotes the cardiovascular subcomponent of the SOFA score. SOFA-C=0 No need for inotrope or vasopressor, mean arterial pressure (MAP) > 70mmHg, SOFA-C =1 MAP < 70mmHg, SOFA-C=2 any dose of dobutamine or dopamine <5 ìg/kg/minute,
{kind=link}
{kind=link}
Further episodes of EMCrit Podcast
Further podcasts by Scott D. Weingart, MD FCCM
Website of Scott D. Weingart, MD FCCM