Podcast 115 – A New Paradigm for Post-Intubation Pain, Agitation, and Delirium (PAD) - a podcast by Scott D. Weingart, MD FCCM
from 2014-01-13T21:00:48
All the way back on Podcast 21, I advocated for better post-intubation sedation in the ED. Well, now it turns out that if you are still using just lorazepam and vecuronium you are now even further from the ideal.
It is all about Sleep and Orientation
Bad sedation strategies destroy sleep architecture and orientation, then patients become crazy.
Delirium=Death
* The impact of delirium in the intensive care unit on hospital length of stay. Intensive Care Med 2001; 27:1892–1900
* Delirium as a predictor of mortality in mechanically ventilated patients in the intensive care unit. JAMA 2004; 291:1753–1762
* Occurrence of delirium is severely underestimated in the ICU during daily care. Intensive Care Med 2009; 35:1276–1280
* Delirium leads to long-term cognitive impairment (N Engl J Med 2013; 369:1306-1316) HT to @icudelirium
* Days of delirium are associated with 1-year mortality in an older intensive care unit population. Am J Respir Crit Care Med 2009; 180:1092–1097
* Deep sedation associated with higher mortality (Critical Care 2015, 19:197 )
It doesn't matter if we screw it up Downstairs, they can Fix it in the ICU
Ummm, not so much if you believe the SPICE Study-In 251 critically ill patients at multiple centers, we identified deep sedation within 4 hours of commencing ventilation as an independent negative predictor of the time to extubation, hospital death, and 180-day mortality. The early phase of ICU sedation is usually unaccounted for in randomized controlled trials due to late randomization. (Am J Respir Crit Care Med Vol 2012;186(8):724–731)[cite source='doi']10.1164/rccm.201203-0522OC[/cite]
A1 Sedation - Analgesia First
Stick your finger down your throat--now leave it there
Strom et al. evaluated this: RCT of 140 patients-analgesia vs. analgesia+sedation. Analgesia only showed shorter vent time and ICU LOS.[cite source='pubmed']20116842[/cite]
Analgosedation: a paradigm shift in intensive care unit sedation practice,[cite source='doi']10.1345/aph.1Q525[/cite].
Just put patients on a fentanyl drip. If not go with dilaudad IV. When remifentanil is cheap, we'll switch to that in a bunch of patient categories.[cite]15329588[/cite]
Then evaluate pain and decide if the patient needs additional pushes of pain meds.
Consider using the Behavioral Pain Scale (Crit Care Med 2001;29(12):2258) HT to Nikolay Yusupov
Myth - We can prevent PTSD if we Black Out the ICU Experience
just the other way around
Myth - Benzos are just Swell
Not so much-Benzos lead to longer length of stay, longer vent time, and increased delirium.
Benzodiazepine versus nonbenzodiazepine-based sedation for mechanically ventilated, critically ill adults: a systematic review and meta-analysis of randomized trials,[cite source='doi']10.1097/CCM.0b013e3182a16898[/cite].
Myth - Short-Acting Sedatives and Analgesics Go Away Quickly
You need a goal, like RASS
Here is the RASS Scale from the amazing ICU Delirium Site
Myth-Pain is a Great Pressor
Patients should never be undersedated due to hemodynamics
Patient Scenarios
Standard Critically Ill Patients
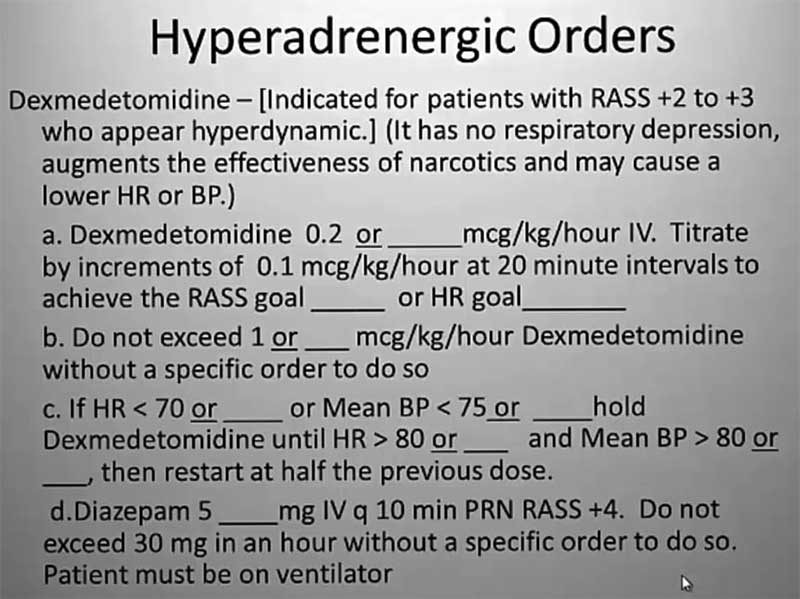
Fentanyl and Dexmedetomidine (or Propofol)
Dan Herr's Method of Dex Titration
Neuro Patients/DTs
{kind=link}
{kind=link}
{kind=link}
Further episodes of EMCrit Podcast
Further podcasts by Scott D. Weingart, MD FCCM
Website of Scott D. Weingart, MD FCCM