Podcast 155 – Status Epilepticus with Tom Bleck - a podcast by Scott D. Weingart, MD FCCM
from 2015-08-14T00:43:03
Today I get to talk Status Epilepticus with Tom Bleck.
Tom Bleck is a neurointensivist from Rush Medical College in Chicago, where he is a professor of neurological sciences, neurosurgery, medicine, and anesthesiology. Dr. Bleck is board certified in internal medicine, with subspecialty certification in critical care medicine; neurology, with subspecialty certification in vascular neurology; clinical neurophysiology; and neurocritical care. He was the founding president of the Neurocritical Care Society.
Here are the questions we discussed:
Initial Treatment
RAMPART [cite source='pubmed']21967361[/cite] showed us that 10 mg IM Midazolam was at least as good as 4 mg IV Lorazepam
If we have an IV, why are we not using IV midazolam over IV Lorazepam?
When is Status Refractory?
* "Status should be considered refractory after the failure of the first agent that should have worked"
* "If you fail lorazepam, you should move to general anesthesia"
* "The longer you seize, the tougher it will be to break"
When should you say that the seizure is unlikely to end? At 5 minutes, you have an 80% or greater chance that you will continue seizing
See Josh Farkas' view on the rapid sequence termination
So if they fail lorazepam (midazolam?), we should consider intubation and general anesthesia.
Which Paralytic?
Sux vs. Roc
Which agent is best for General Anesthesia?
High Dose Midazolam (Neurology 2014;82:359)
– loading dose: 0.2 mg/kg
– maintenance: 0.1 - 2.0 mg/kg/hr
Propofol
may be bad (Prasad A et al Epilepsia 2001;?42:380-386)
Conventional AEDs
Which one and when?
* Fosphenytoin
* Valproic Acid
* Levetiracetam (Keppra)
* Lacosamide
Dr. Bleck recommends one of the latter two. Levetiracetam at a dose of 1 gm, may repeat 1-2 times or Lacosamide 200-300 mg.
Still Refractory
* Ketamine for Status [cite source='pubmed']23758557[/cite] and this article. Reasonable Starting Dose 3-5 mg/kg.
* Hypothermia
* Inhaled General Anesthesia-AnaConDa with Iso or Desflurane
* This Review Article Discusses Super-Refractory Status Management
EEGs
When should a patient get continuous EEGs?
What if you don't have access
EEG Interpretation for Dummies
* EEG should be the opposite of your EKG (Vfib is good)
* Reactive is better than non-reactive
What if we can't get one?
NitWitticism: Being in burst suppression will prevent you from seizing. Pts can seize through burst. May need to be made flatline EEG.
Etiology
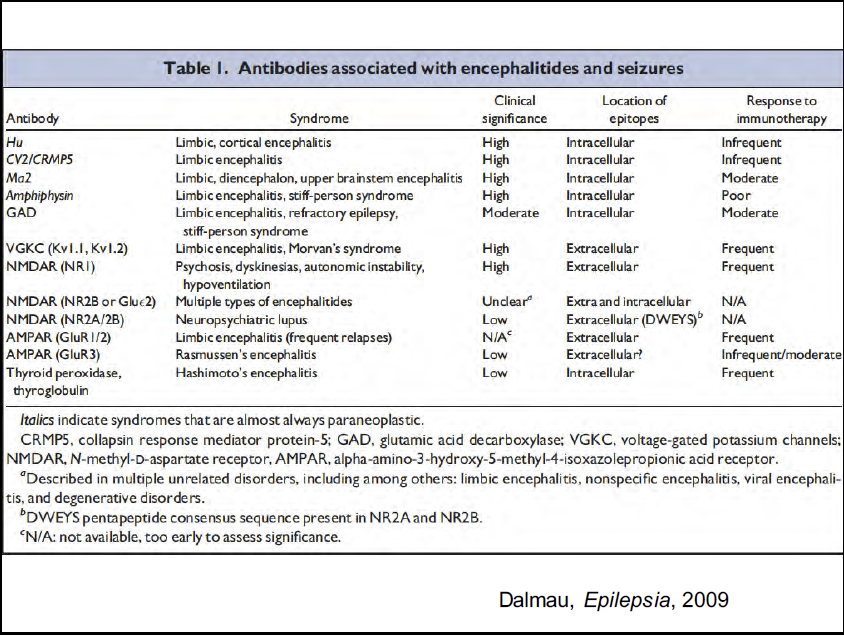
Consider Autoimmune Encephalitis, especially Anti-NMDA Encephalitis (Neurology 2015 vol. 85 no. 18 1604-1613)
Consider Tox
* INH
* Tricyclics
* Theophylline
* Cocaine
* Alcohol/Benzo withdrawal
* Organophosphates
More from Tom on Status
* Rossetti and Bleck in ICM
* Tom Bleck's Slides from SMACC on SE
* EMCrit Podcast
{kind=link}
{kind=link}
Further podcasts by Scott D. Weingart, MD FCCM
Website of Scott D. Weingart, MD FCCM