Podcast 170 – the ER REBOA Catheter with Joe DuBose - a podcast by Scott D. Weingart, MD FCCM
from 2016-03-21T16:49:42
We've discussed REBOA before on the EMCrit Podcast with Megan Brenner. We also featured the first prehospital REBOA case. It was an interesting treatment, but an extremely complex one. That has all changed with the new ER REBOA catheter.
In this podcast, I discuss the new catheter from Prytime and then I interview Dr. Joe DuBose, a trauma and vascular surgeon who performed the first ER REBOA placement that resulted in a survivor.
Conflicts of Interest
Neither Dr. DuBose nor I have any conflicts of interest regarding the ER REBOA catheter or otherwise
Slides from Dr. DuBose's Case
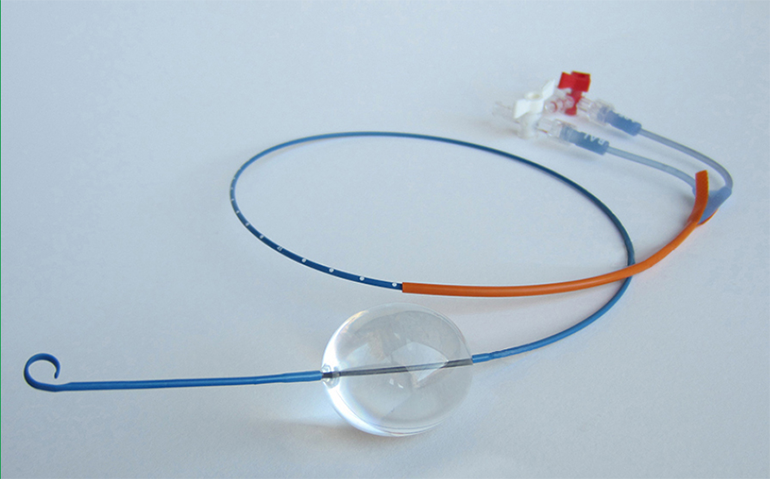
ER REBOA Visual Tour
ER REBOA Placement Video
Steps to Placement of the ER REBOA Catheter
Gain Access to the Common Femoral Artery with a 7-French Introducer
* Just like normal for an arterial line, except make sure you are hitting common femoral and not superficial femoral artery. The point of entry should be 2 cm below inguinal ligament (estimate ligament by anterior superior iliac to pubic tubercle). This may be much higher than you are used to.
* Only some introducers will work:
Attach a Syringe to the Balloon Port of the REBOA Catheter
* Use a 25 or 30 ml syringe, filled with 24 ml of NS
Test the Balloon
* Inflate to test patency
* Make sure to fully deflate the balloon. Apply some extra suction to really shrink it down and then lock the balloon stopcock
Attach Transducer
* Attach a pressure transducer to the arterial line port. Zero the transducer to the phlebostatic access
Measure externally
* Zone 1 is measured with the proximal edge of the balloon at the xiphoid, Zone 3 is measured with the proximal edge of the balloon just above the umbilicus.
from J Trauma. 2011 Dec;71(6):1869-72
Insert the REBOA Catheter
* Use the orange sheath to straighten the p-tip
* Insert the orange sheath 1cm into the valve of the 7-french introducer
* Advance the REBOA catheter a few cm into the introducer
* Pull back on the orange sheath
* Advance the REBOA catheter to the predetermined depth
Inflate the Balloon
* Hold the REBOA catheter to prevent it from pushing out
* Open the Stopcock
* Inflate until resistance goes to moderate or the blood pressure on the arterial line tracing of the REBOA Catheter starts to increase. In general, this corresponds to 12-22 mls depending on the size of the aorta–but this must be individualized to the patient. The actual inflation is far harder than you may think. For me, it is the maximal force I can apply with 1 hand.
* Never instill more than 24 mls. Never more than 24
* Close the stopcock
Secure the Catheter
* If the catheter is not secured externally it will migrate out from aortic pressure, especially in zone I
* It will be an institution dependent choice as to how to ...
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Further episodes of EMCrit Podcast
Further podcasts by Scott D. Weingart, MD FCCM
Website of Scott D. Weingart, MD FCCM