Podcast 181 – Pulmonary Hypertension and Right Ventricular Failure with Susan Wilcox - a podcast by Scott D. Weingart, MD FCCM
from 2016-09-05T17:46:41
The Right Ventricle gets no respect, but it is an easy source of clean kills in the ED. We haven't covered pulmonary hypertension and acute on chronic RV failure on the show yet--we need to fix that ASAP. So, let's hear from Susan Wilcox, MD on this critical topic. She just wrote an amazing review on the subject for Ann Emerg Med and as an EM Intensivist, she is the perfect person to talk on this topic.
Best Current Review for EM
* Ann Emerg Med 2015;66(6):619 by Susan R. Wilcox, MD
Other Articles to Check Out
* Inten Care Med 2014;40:1930
* 21700906
* Crit Care Clin 2014;30:475
* CCR-4-49
* DOI 10.1111/anae.12831
Note: A good portion of these shownotes were contributed by Gregg Chesney, MD; ED Intensivist
Some Info
RV function determined by 3 P’s: preload, pump (RV contractility), and pipes (afterload)
RV is different than LV
* Thin walled, less muscular, more compliant, working against less afterload (PVR 1/10 of SVR)
* More dependent on volume loading than pressure to accomplish work of ventricle
* LV contracts in a wringing motion, RV contracts in a longitudinal up-and-down motion and compresses medially against septum
* RV doesn’t adapt well to acute changes in pressure/volume à dilates and becomes stiffer (takes 96 hrs to adapt)
Ventricular interdependence = LV and RV function are dependent on one another.
* LV preload = RV stroke volume, failing RV = decreased LV preload
* LV and RV share a muscular septum - contributes 20-40% of the work of RV contraction when LV contracts
* Dilated failing RV pushes IV septum into LV impairing LV filling/contractility and also impairing role of RV septum on RV contractility
RV Spiral Of Death
RV ischemia is the common final pathway that contributes to progressively worsening acute RV failure
Types of Pulmonary Hypertension
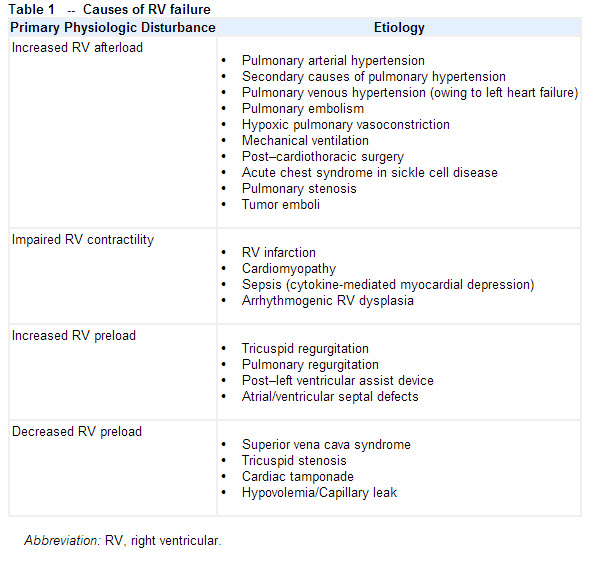
Causes of RV Failure can be broken into 4 Categories
from King et al
ECHO: How to evaluate for RV failure at bedside
* Apical 4 chamber to evaluate relative size of RV to LV and to evaluate how RV “looks”
* If you are skilled, focus on lateral tricuspid annulus movement (TAPSE) 1.6
* McConnell’s sign may be indicative of acute RV failure with RV ischemia, not just seen in acute PE
* Parasternal short at level of mid-papillary to eval relationship between volumes and size of LV and RV and intraventricular septum – look for septal shift and the "D" Sign
* Plethoric IVC regardless of volume Status
* As RV dilates in chronic failure, there will be disruption of the tricuspid annulus leading to tricuspid regurg
Six step approach to management of acute RV failure
Step 1: Optimize volume status
* Lasix vs. fluids, use PSAX echo view to decide
* Err on the side of volume constriction, they are often overloaded unless the patient has a known source of volume loss
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Further episodes of EMCrit Podcast
Further podcasts by Scott D. Weingart, MD FCCM
Website of Scott D. Weingart, MD FCCM