Podcast 187 – Hypernatremia (Uggggh!) - a podcast by Scott D. Weingart, MD FCCM
from 2016-11-28T17:24:56
So we've discussed hyponatremia a ton on the blog site. That's because hyponatremia has become a little bit sexy. Not so with sodium that is too high. But I've seen a bunch of less than ideal management of hypernatremia, so I figured it is time to put out a podcast about it. This is mostly so I have a place to go to look all of this up.
Join us at the EMCrit Conference Jan 11 2017
EMCrit Conference Site
Articles
* Androgue-Madias from NEJM
* Hypo and Hypernatremia in the Crit Ill
* Hypernatremia in the Critically Ill
Read this Book
* Joel Topf is of PBF is 2nd author of an excellent fluids and electrolyte text. He has released it for free on the Precious Body Fluids Blog
How do you become Hypernatremic
Loss of free water and/or
Loss of hypotonic fluid and/or
Increased Solute and
thirst or access to water must be thwarted
Hypernatremia Results in...
* Impaired glucose metabolism
* Rhabdo
* AMS
* Seizures
Avoid Iatrogenic Complications
Cerebral Shrinkage is Bad
Causes of Hypernatremia
Extrarenal water loss
* Dehydration by exposure
* Burns
* Gastric losses
* Diarrhea (Lactulose)
* Fever
Salt gain
* Infusion of sodium-rich fluids of some sort (eg. hypertonic saline)
* Ingestion of sea water
* Salt pica
Nephrogenic DI
* Hypercalcemia
* hypokalemia
* Lithium
* Pyelonephritis
* Medullary sponge kidney
* Multiple myeloma
* Amyloid
* Sarcoid
Central DI
* Traumatic brain injury
* Pituitary tumour
* Meningitis
* Encephalitis
* Tuberculosis
* Sarcoidosis
* Idiopathic
* ICH
Renal losses
* Glucosuria
* Mannitol
* Urea therapy
* Loop diuretics
* Post obstructive diuresis
* Hyperaldosteronism
* Cushings
This table stolen directly from Deranged Physiology (primarily b/c I hate making html tables)
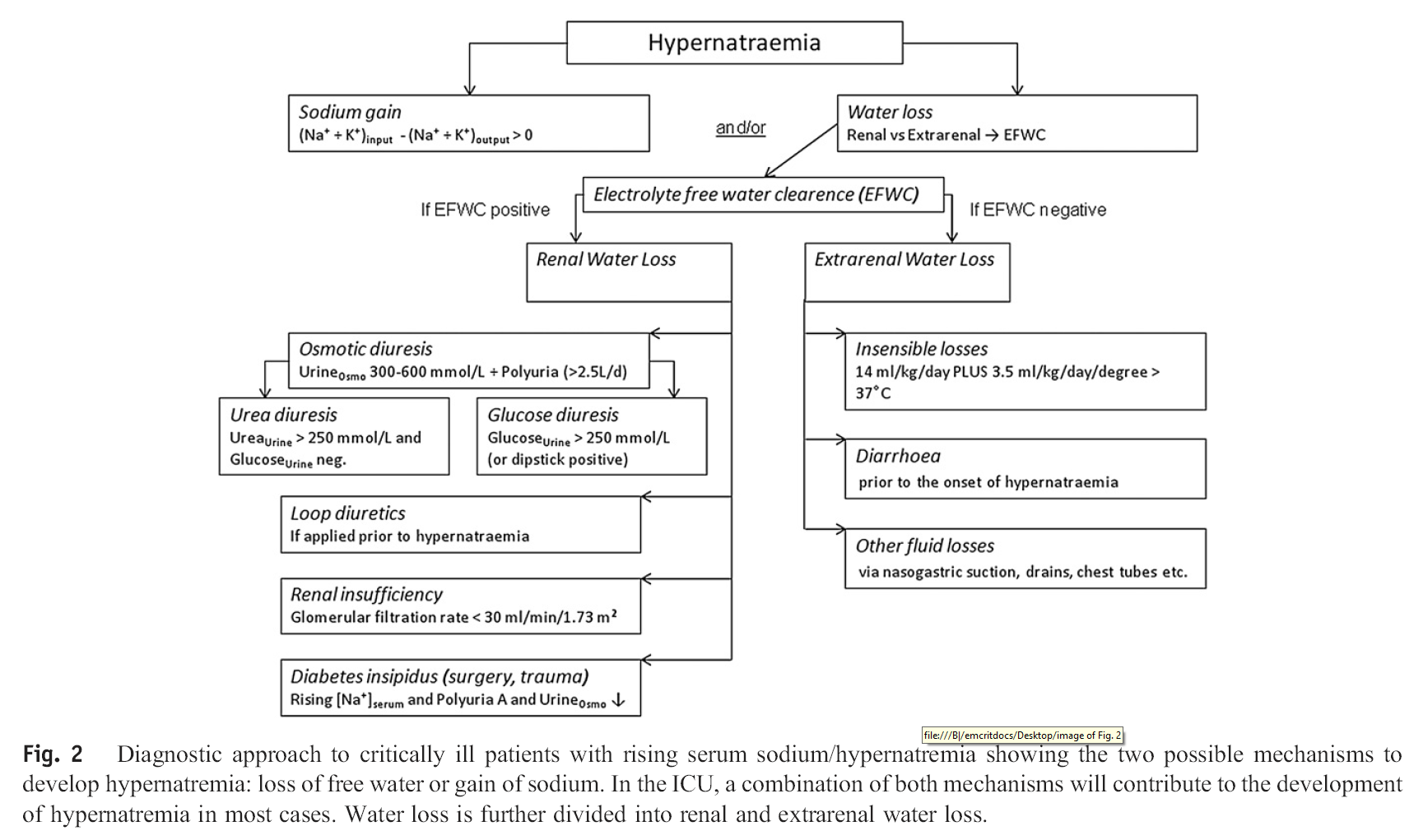
Chart of Figuring Out What the Hell is Going On
from Lindner et al article linked above
Treatment
Stop or Correct the Underlying Cause
Correct Quickly if Na got high superrapid-style (Idiots drinking a quart of soy sauce)
Correct < 10 meq/day (< 0.5 mmol/L/hr) if the Na went up gradually (2-3 mmol/L/hr if rapid rise in sodium)
Oral/Gastric Tube is the safest way to correct
Administer Hypotonic Fluids (D5W, 1/4 NS, 1/2 NS, sterile water (central line))
Do not administer NS unless pt is HYPOVOLEMIC (NS doesn't work!!!; see Androgue-Madias for mathematical demonstration of this)
{kind=link}
{kind=link}
{kind=link}
Further episodes of EMCrit Podcast
Further podcasts by Scott D. Weingart, MD FCCM
Website of Scott D. Weingart, MD FCCM