Podcast 85 – A Confirmation of Prejudices: Chloride and Pressure Poisoning - a podcast by Scott D. Weingart, MD FCCM
from 2012-10-29T22:05:11
In this Hurricane Sandy episode of the EMCrit podcast, I talk about the confirmation of two of my clinical prejudices.
Chloride Poisoning
So I've always preached that grabbing normal saline for every ED patient is poor thinking and poor practice. We discussed this topic in the 4th Acid-Base Podcast on Fluids. Up until now, I did not have great evidence for my prejudice; now at least, I have reasonably good evidence:
Major complications, mortality, and resource utilization after open abdominal surgery: 0.9% saline compared to Plasma-Lyte (Ann Surg. 2012 May;255(5):821-9)
Association Between a Chloride-Liberal vs Chloride-Restrictive Intravenous Fluid Administration Strategy and Kidney Injury in Critically Ill Adults (JAMA. 2012 Oct 17;308(15):1566-72)
Definitive? Nope, but it just seems like good medicine to treat fluids like any other drug and actually choose the ideal one for the clinical situation.
Resus.me Post: What’s with all the chloride? An assault on salt | Resus M.E!
Upate:
Association Between the Choice of IV Crystalloid and In-Hospital Mortality Among Critically Ill Adults With Sepsis
Karthik Raghunathan (Crit Care Med 2014 citation pending)
A Diversion on Osmolality
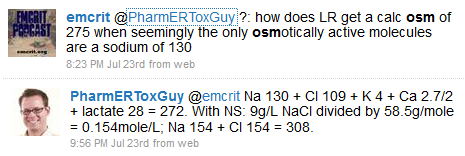
Peter Sherren made a great comment in the podcast on the Brain Code regarding my statement that lactated ringers is an inappropriate fluid in high ICP. So I had a bit of a think on the topic and then was baffled as to why LR has a Na of 130 and yet a Osm of 272-5.
Brian Hayes responded to a tweet on the topic with what is probably self-evident to everyone but me: the Osm calculation we use is actually a crappy short cut; all components of a fluid need to be calculated to get the real Osm. Yet, when I thought about this still further, I realized that what is written on the bag is not actually the in-vivo Osm effects. Instead, the Na is probably the key.
Want proof of this concept? D5W has an Osm of 252 on the bag, but the effective Osm is 0 as soon as your cells take up the glucose.
So can you use LR in high ICP, yes probably not too big a deal, but the net Osm effects will probably be to lower the serum Na and Osm. If you buy choosing the ideal fluid for acid-base, it probably makes sense to choose the ideal fluid for Osm as well. Maybe this prejudice will be verified 5 years from now with a real article.
Here is the article I mentioned on the Osm effects of LR on healthy volunteers: (Anesth Analg 1999;88:999 –1003)
Here is an Osm calculator from GlobalRPH.
A Diversion on the need for Conversion of the Buffer Bases
Want what I think is the ideal resus fluid? Mix this on the fly:
Ultimate Resus Fluid? 1 amp of 44.6 bicarb in 500 ml of NS makes 550 of total volume= Na 121.6 Cl 77 Bicarb 44.6 to extended out to 1 liter= Na 217 Cl 138.6 BiCarb 80 1.3% Balanced Saline solution
There is ABSOLUTELY no evidence for this. If someone wants to do the study,
{kind=link}
Further episodes of EMCrit Podcast
Further podcasts by Scott D. Weingart, MD FCCM
Website of Scott D. Weingart, MD FCCM