Podcast 86 – IVC Ultrasound for Fluid Tolerance in Spontaneously Breathing Patients – EAT IT STONE - a podcast by Scott D. Weingart, MD FCCM
from 2012-11-12T00:23:36
Can the Inferior Vena Cava Ultrasound guide our fluid administration in the ED? Of course it can!
So I was getting on the plane to Las Vegas for Essentials 2012, on my iphone was the latest from Mike and Matt of the Ultrasound Podcast. Up pops Mike "the Rock" Stone interviewing my buddy, Haney Mallemat; these two ultrasound gurus discuss some ultrasound soundbites, but then... They both state that IVC ultrasound is useless for determining fluid responsiveness. It is worth taking a listen to that episode if you have a moment. So how can two brilliant guys get it so wrong? They just had their focus knob turned all the way to the right. Lets optimize their settings with an EMCrit Podcast.
Mechanically Vented Patients
Now, most of the podcast bashed IVC in spont breathing patients, but there was some overflow disparaging of IVC in mech vented patients, so let's get that out of the way first. There is plenty of literature for these patients. Put them on a temporary, high tidal volume (10 ml/kg). Get an IVC shot and if it increases in size by 15-18% (depending on the study), the patient is fluid responsive.
* Intensive Care Med. 2004 Sep;30(9):1740
* Intensive Care Med. 2004 Sep;30(9):1834
* Neurocrit Care. 2010;13:3
* J Trauma. 2007;63:495
* J Intensive Care Med. 2011 Mar-Apr;26(2):116
Spontaneously Breathing Patients
Now as the two ultrasound masters allude to, there have been a few studies showing IVC ultrasound assessment merely correlates with CVP (it actually correlates with respirophasic CVP) and then use that fact to write off the IVC. Now we have maligned CVP as a marker of fluid responsiveness so IVC is crap as well, right?
There is evidence for the use of IVC as a marker of fluid status. In patients with ultrafiltration for congestive heart failure (Intensive Care Med. 2010 Apr;36(4):692-6) as well as fluid removal during hemodialysis (Clin J Am Soc Nephrol 2006;1:749 and Nephrol Dial Trans 1989;4:563). There was also a trauma study showing that fluid resuscitated patients with IVC collapse were more likely than those without to have recurrent hypotension (J Trauma. 2007 Dec;63(6):1245).
There was also a study just published in the Aussie EM Journal. This study was severely limited by the fact that none of these patients had any significant IVC collapse and the criterion standard is not a test any of us consider useful for cardiac index measurements; further, looking at the tables, some of the responder group did not seem to have any sig. increase in their CI in response to fluid. (Emerg Med Aust 2012;24:534).
And a meta-analysis study showing IVC's relation to fluid status (AJEM 2012;30:1414).
Luckily, there was also a recently published study with the table below (Crit Care 2012;16:R188).
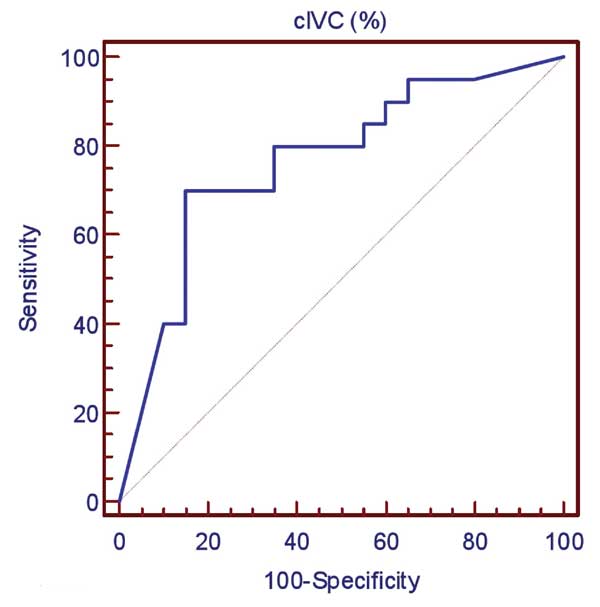
Here is figure 1 from the study
Here is the area under the cure (AUC); you notice there are points with much higher specificity.
Update:
Hot off the presses, this study is more reassuring: (Shock 2013;39(2):155)
It lends additional credence to the use of dynamic IVC for fluid responsiveness.
It's not Fluid Responsiveness, It's Fluid Tolerance!
This is the crux of the matter. In the ED, we want to give a bunch of fluid, but not if we are going to cause pulmonary edema. The term, fluid tolerance, is a perfect description of this idea. Responsiveness is great, but all we want to make sure of is that we are not going to d...
{kind=link}
{kind=link}
Further episodes of EMCrit Podcast
Further podcasts by Scott D. Weingart, MD FCCM
Website of Scott D. Weingart, MD FCCM