Practical Evidence Podcast 015 – Surviving Sepsis Campaign (SSC) Guidelines 2016 (in 2017) - a podcast by Scott D. Weingart, MD FCCM
from 2017-01-22T18:47:38
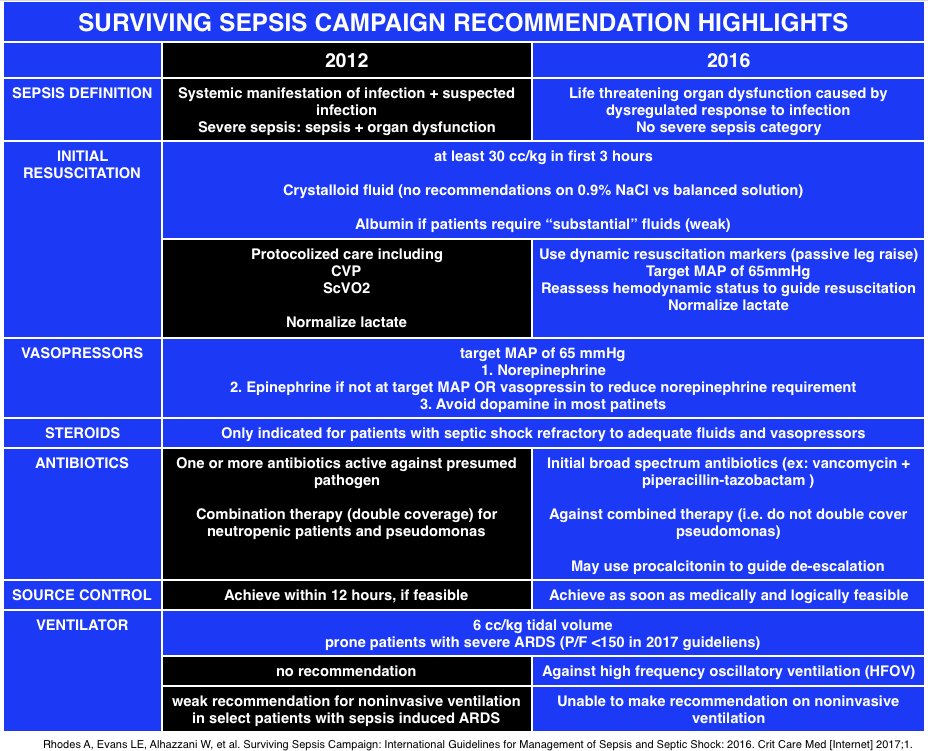
Image Taken from the FOAMCast Episode
We've discussed SEPSIS a ton on EMCrit.
* Podcast 154 - Preemptive Sepsis Panel SmaccBack
* Wee - Cliff Deutschman with Additional Thoughts on Sepsis 3.0
* Renoresuscitation: Sepsis resuscitation designed to avoid long-term complications
* Podcast 112 - A Response to the Marik Sepsis Fluids Lecture
* Podcast 169 - Sepsis 3.0 with Merv Singer
* Podcast 89 - Lessons from the STOP Sepsis Collaborative
Recently, the Surviving Sepsis Campaign released their 2016 guideline update. Overall, I think this iteration moves the guidelines closer to the best evidence out there. Of course, when you travel that path it forces a divergence from the distinctly non-evidence-based CMS guidelines. In this Practical Evidence Podcast, we will discuss the SSC guidelines, the aforementioned divergence, and various alcohol recommendations. I brought on my buddy, Jeremy Faust, to discuss the changes. Jeremy is 1/2 of the FOAMcast podcast which just discussed the new guidelines in a recent episode.
Guideline Stuff
* The SSC 2016 Guidelines
* PDF Version of the SSC 2016
* Users' Guide to the Guidelines
* Our Emergency Medicine Clinics Article
The Guideline Recommendations
The Definition of Sepsis
They basically ratified SEPSIS 3.0
(Jeremy found where he saw the remnants of the old definition; it was in the Users' guide figure 2--super contradictory)
Fluids
30 ml/kg in the first 3 hours
Crystalloid first, then maybe albumin
Use dynamic markers and/or fluid challenges
Goal MAP>65
EGDT is no longer recommended
Lactate
attempt to normalize lactate
Blood Cultures
get them before antibiotics, if obtaining them will not delay the provision of antibiotics
Antibiotics
Within 1 hour of sepsis or septic shock
Vasopressors
Norepi is the first choice, add in epi or vaso
Do not use dopamine
Steroids
200 mg Hydrocortisone for patients who are still unstable after fluids and vasopressors
Blood
In most circumstances, use a trigger of <7.0 g/dL
{kind=link}
{kind=link}
Further episodes of EMCrit Podcast
Further podcasts by Scott D. Weingart, MD FCCM
Website of Scott D. Weingart, MD FCCM